What is cirrhosis?
Cirrhosis is a condition in which the liver slowly deteriorates and is unable to function normally due to chronic, or long lasting, injury. Scar tissue replaces healthy liver tissue and partially blocks the flow of blood through the liver.
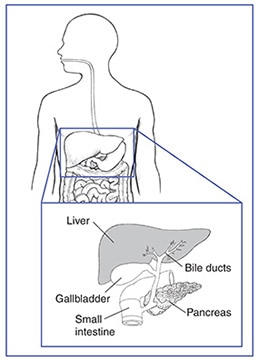
The liver is the body’s largest internal organ. The liver is called the body’s metabolic factory because of the important role it plays in metabolism—the way cells change food into energy after food is digested and absorbed into the blood. The liver has many functions, including
- taking up, storing, and processing nutrients from food—including fat, sugar, and protein—and delivering them to the rest of the body when needed
- making new proteins, such as clotting factors and immune factors
- producing bile, which helps the body absorb fats, cholesterol, and fat-soluble vitamins
- removing waste products the kidneys cannot remove, such as fats, cholesterol, toxins, and medications
A healthy liver is necessary for survival. The liver can regenerate most of its own cells when they become damaged. However, if injury to the liver is too severe or long lasting, regeneration is incomplete, and the liver creates scar tissue. Scarring of the liver, also called fibrosis, may lead to cirrhosis.
The buildup of scar tissue that causes cirrhosis is usually a slow and gradual process. In the early stages of cirrhosis, the liver continues to function. However, as cirrhosis gets worse and scar tissue replaces more healthy tissue, the liver will begin to fail. Chronic liver failure, which is also called end-stage liver disease, progresses over months, years, or even decades. With end-stage liver disease, the liver can no longer perform important functions or effectively replace damaged cells.
Cirrhosis is the 12th leading cause of death in the United States, accounting for nearly 32,000 deaths each year. More men die of cirrhosis than women.1
What causes cirrhosis?
Cirrhosis has various causes. Many people with cirrhosis have more than one cause of liver damage.
The list below shows common causes of cirrhosis in the United States.2 While chronic hepatitis C and alcohol-related liver disease are the most common causes of cirrhosis, the incidence of cirrhosis caused by nonalcoholic fatty liver disease is rising due to increasing rates of obesity.
Most Common Causes of Cirrhosis
Chronic hepatitis C. Hepatitis C is due to a viral infection that causes inflammation, or swelling, and damage to the liver. The hepatitis C virus spreads through contact with infected blood, such as from a needlestick accident, injection drug use, or receiving a blood transfusion before 1992. Less commonly, hepatitis C can be spread by sexual contact with an infected person or at the time of childbirth from an infected mother to her newborn.
Hepatitis C often becomes chronic, with long-term persistence of the viral infection. Chronic hepatitis C causes damage to the liver that, over years or decades, can lead to cirrhosis. Advanced therapies for chronic hepatitis C now exist, and health care providers should treat people with chronic hepatitis C before they develop severe fibrosis or cirrhosis. Unfortunately, many people first realize they have chronic hepatitis C when they develop symptoms of cirrhosis. More information is provided in the NIDDK health topic, Hepatitis C.
Alcohol-related liver disease. Alcoholism is the second most common cause of cirrhosis in the United States. Most people who consume alcohol do not suffer damage to the liver. However, heavy alcohol use over several years makes a person more likely to develop alcohol-related liver disease. The amount of alcohol it takes to damage the liver varies from person to person. Research suggests that drinking two or fewer drinks a day for women and three or fewer drinks a day for men may not injure the liver.3 Drinking more than these amounts leads to fat and inflammation in the liver, which over 10 to 12 years can lead to alcoholic cirrhosis.4
Nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH). In NAFLD, fat builds up in the liver; however, the fat buildup is not due to alcohol use. When the fat accompanies inflammation and liver cell damage, the condition is called nonalcoholic steatohepatitis, or NASH, with “steato” meaning fat, and “hepatitis” meaning inflammation of the liver. The inflammation and damage can cause fibrosis, which eventually can lead to cirrhosis.
Extra fat in the liver has many causes and is more common in people who
- are overweight or obese.
- have diabetes—a condition characterized by high blood glucose, also called high blood sugar.
- have high blood cholesterol and triglycerides, called hyperlipidemia.
- have high blood pressure.
- have metabolic syndrome—a group of traits and medical conditions linked to being overweight and obese that makes people more likely to develop both cardiovascular disease and type 2 diabetes. Metabolic syndrome is defined as the presence of any three of the following: large waist size, high triglycerides in the blood, abnormal levels of cholesterol in the blood, high blood pressure, and higher than normal blood glucose levels. NASH may represent the liver component of the metabolic syndrome.
NASH now ranks as the third most common cause of cirrhosis in the United States. More information is provided in the NIDDK health topic, Nonalcoholic Steatohepatitis.
Chronic hepatitis B. Hepatitis B, like hepatitis C, is due to a viral infection that causes inflammation and damage to the liver. Chronic infection can lead to damage and inflammation, fibrosis, and cirrhosis. The hepatitis B virus spreads through contact with infected blood, such as by needlestick accident, injection drug use, or receiving a blood transfusion before the mid-1980s. Hepatitis B also spreads through sexual contact with an infected person and from an infected mother to child during childbirth.
In the United States, hepatitis B is somewhat uncommon, affecting less than 1 percent of the population, or fewer than one in 100 people.5 In many areas of the world, however, hepatitis B is common. In some parts of Africa and in most of Asia and the Pacific Islands, about 5 to 7 percent of the population has chronic hepatitis B. In some parts of Africa, more than 8 percent of the population has chronic hepatitis B.6 For these reasons, hepatitis B is likely the major cause of cirrhosis worldwide. However, in the United States, hepatitis B ranks well behind hepatitis C, alcohol-related liver disease, and NASH.
Therapies for chronic hepatitis B now exist and health care providers should treat people with chronic hepatitis B before they develop severe fibrosis or cirrhosis. Unfortunately, many people first realize they have chronic hepatitis B when they develop symptoms of cirrhosis.
Hepatitis B is also a preventable disease. Since the 1980s, a hepatitis B vaccine has been available and should be given to newborns and children in the United States. Adults at higher risk of getting hepatitis B should also get the vaccine. More information is provided in the NIDDK health topics, Hepatitis B and Hepatitis B: What Asian and Pacific Islander Americans Need to Know.
Less Common Causes of Cirrhosis
Less common causes of cirrhosis include the following:
Autoimmune hepatitis. In this form of hepatitis, the body’s immune system attacks liver cells and causes inflammation, damage, and eventually cirrhosis. Normally, the immune system protects people from infection by identifying and destroying bacteria, viruses, and other potentially harmful foreign substances. In autoimmune diseases, the body’s immune system attacks the body’s own cells and organs. Researchers believe genetics, or inherited genes, may make some people more likely to develop autoimmune diseases. At least 70 percent of those with autoimmune hepatitis are female.7 More information is provided in the NIDDK health topic, Autoimmune Hepatitis.
Diseases that damage, destroy, or block the bile ducts. Several diseases can damage, destroy, or block the ducts that carry bile from the liver to the small intestine, causing bile to back up in the liver and leading to cirrhosis. In adults, the most common of these diseases is primary biliary cirrhosis, a chronic disease that causes the small bile ducts in the liver to become inflamed and damaged and ultimately disappear. Primary sclerosing cholangitis is a disease that causes irritation, scarring, and narrowing of the larger bile ducts of the liver.
In infants and children, causes of damage to or disappearance of bile ducts that can lead to cirrhosis include
- Alagille syndrome, a collection of symptoms that indicates a genetic digestive disorder and leads to a loss of bile ducts in infancy.
- biliary atresia, a life-threatening condition that affects newborns in which bile ducts are missing. The cause is unknown. Biliary atresia is the most common reason for liver transplantation in children.8
- cystic fibrosis, an inherited disease of the lungs, intestines, pancreas, and bile ducts in which the body does not produce enough fluid and mucus becomes thick and blocks off small bile ducts. This blockage of the bile ducts can lead to cirrhosis.
Long-term blockage of the bile ducts by gallstones can cause cirrhosis. Cirrhosis may also develop if the bile ducts are mistakenly tied off or injured during surgery on the gallbladder or liver.
Inherited diseases that affect the liver. Inherited diseases that interfere with how the liver produces, processes, and stores enzymes, proteins, metals, and other substances can cause cirrhosis. These diseases include alpha-1 antitrypsin deficiency, hemochromatosis, Wilson disease, galactosemia, and glycogen storage diseases. More information is provided in the NIDDK health topics:
Rare viral infections of the liver. Hepatitis D, or hepatitis delta, and hepatitis E are two rare viral infections of the liver. Hepatitis D infection occurs only in people who have hepatitis B. People infected with chronic hepatitis B and chronic hepatitis D are more likely to develop cirrhosis than people infected with chronic hepatitis B alone.9
Hepatitis E is a virus found in domestic and wild animals, particularly pigs, and can cause hepatitis in humans. People with weakened immune systems, including people who are liver or kidney transplant recipients or who have acquired immune deficiency syndrome (AIDS), can develop chronic hepatitis E. Chronic hepatitis E can cause scarring of the liver and cirrhosis. Current treatments for chronic hepatitis D and E are experimental and only partially effective.
Other causes. Other causes of cirrhosis may include
- reactions to medications taken over a period of time.
- prolonged exposure to toxic chemicals.
- parasitic infections.
- chronic heart failure with liver congestion, a condition in which blood flow out of the liver is slowed. Liver congestion can also occur after surgery to correct a congenital heart problem—a heart problem that is present at birth.
Trauma to the liver or other acute, or short term, causes of damage do not cause cirrhosis. Usually, years of chronic injury are required to cause cirrhosis.
What are the signs and symptoms of cirrhosis?
Many people with cirrhosis have no symptoms in the early stages of the disease. However, as the disease progresses, a person may experience the following symptoms:
- fatigue, or feeling tired
- weakness
- itching
- loss of appetite
- weight loss
- nausea
- bloating of the abdomen from ascites—a buildup of fluid in the abdomen
- edema—swelling due to a buildup of fluid—in the feet, ankles, or legs
- spiderlike blood vessels, called spider angiomas, on the skin
- jaundice, a condition that causes the skin and whites of the eyes to turn yellow
What are the complications of cirrhosis?
As the liver fails, complications may develop. In some people, complications may be the first signs of the disease. Complications of cirrhosis may include the following:
Portal hypertension. The portal vein carries blood from the stomach, intestines, spleen, gallbladder, and pancreas to the liver. In cirrhosis, scar tissue partially blocks the normal flow of blood, which increases the pressure in the portal vein. This condition is called portal hypertension. Portal hypertension is a common complication of cirrhosis. This condition may lead to other complications, such as
- fluid buildup leading to edema and ascites
- enlarged blood vessels, called varices, in the esophagus, stomach, or both
- an enlarged spleen, called splenomegaly
- mental confusion due to a buildup of toxins that are ordinarily removed by the liver, a condition called hepatic encephalopathy
Edema and ascites. Liver failure causes fluid buildup that results in edema and ascites. Ascites can lead to spontaneous bacterial peritonitis, a serious infection that requires immediate medical attention.
Varices. Portal hypertension may cause enlarged blood vessels in the esophagus, stomach, or both. These enlarged blood vessels, called esophageal or gastric varices, cause the vessel walls to become thin and blood pressure to increase, making the blood vessels more likely to burst. If they burst, serious bleeding can occur in the esophagus or upper stomach, requiring immediate medical attention.
Splenomegaly. Portal hypertension may cause the spleen to enlarge and retain white blood cells and platelets, reducing the numbers of these cells and platelets in the blood. A low platelet count may be the first evidence that a person has developed cirrhosis.
Hepatic encephalopathy. A failing liver cannot remove toxins from the blood, so they eventually accumulate in the brain. The buildup of toxins in the brain is called hepatic encephalopathy. This condition can decrease mental function and cause stupor and even coma. Stupor is an unconscious, sleeplike state from which a person can only be aroused briefly by a strong stimulus, such as a sharp pain. Coma is an unconscious, sleeplike state from which a person cannot be aroused. Signs of decreased mental function include
- confusion
- personality changes
- memory loss
- trouble concentrating
- a change in sleep habits
Metabolic bone diseases. Some people with cirrhosis develop a metabolic bone disease, which is a disorder of bone strength usually caused by abnormalities of vitamin D, bone mass, bone structure, or minerals, such as calcium and phosphorous. Osteopenia is a condition in which the bones become less dense, making them weaker. When bone loss becomes more severe, the condition is referred to as osteoporosis. People with these conditions are more likely to develop bone fractures.
Gallstones and bile duct stones. If cirrhosis prevents bile from flowing freely to and from the gallbladder, the bile hardens into gallstones. Symptoms of gallstones include abdominal pain and recurrent bacterial cholangitis—irritated or infected bile ducts. Stones may also form in and block the bile ducts, causing pain, jaundice, and bacterial cholangitis.
Bruising and bleeding. When the liver slows the production of or stops producing the proteins needed for blood clotting, a person will bruise or bleed easily.
Sensitivity to medications. Cirrhosis slows the liver’s ability to filter medications from the blood. When this slowdown occurs, medications act longer than expected and build up in the body. For example, some pain medications may have a stronger effect or produce more side effects in people with cirrhosis than in people with a healthy liver.
Insulin resistance and type 2 diabetes. Cirrhosis causes resistance to insulin. The pancreas tries to keep up with the demand for insulin by producing more; however, extra glucose builds up in the bloodstream, causing type 2 diabetes.
Liver cancer. Liver cancer is common in people with cirrhosis. Liver cancer has a high mortality rate. Current treatments are limited and only fully successful if a health care provider detects the cancer early, before the tumor is too large. For this reason, health care providers should check people with cirrhosis for signs of liver cancer every 6 to 12 months. Health care providers use blood tests, ultrasound, or both to check for signs of liver cancer.
Other complications. Cirrhosis can cause immune system dysfunction, leading to an increased chance of infection. Cirrhosis can also cause kidney and lung failure, known as hepatorenal and hepatopulmonary syndromes.
How is cirrhosis diagnosed?
A health care provider usually diagnoses cirrhosis based on the presence of conditions that increase its likelihood, such as heavy alcohol use or obesity, and symptoms. A health care provider may test for cirrhosis based on the presence of these conditions alone because many people do not have symptoms in the early stages of the disease. A health care provider may confirm the diagnosis with
- a medical and family history
- a physical exam
- a blood test
- imaging tests
- a liver biopsy
Medical and family history. Taking a medical and family history is one of the first things a health care provider may do to help diagnose cirrhosis. He or she will ask the patient to provide a medical and family history.
Physical exam. A physical exam may help diagnose cirrhosis. During a physical exam, a health care provider usually
- examines a patient’s body
- uses a stethoscope to listen to sounds in the abdomen
- taps on specific areas of the patient’s body
The health care provider will perform a physical exam to look for signs of the disease. For example, the liver may feel hard or ascites may cause the abdomen to enlarge.
Blood test. A blood test involves drawing blood at a health care provider’s office or a commercial facility and sending the sample to a lab for analysis. Blood tests can show abnormal liver enzyme levels or abnormal numbers of blood cells or platelets.
Blood tests can help find the cause in people with diagnosed cirrhosis. For example, a health care provider may use blood tests to diagnose hepatitis B and C.
Health care providers use three blood tests to measure the severity of cirrhosis:
- bilirubin, which tests the amount of bile pigment in the blood
- creatinine, which tests kidney function
- international normalized ratio, which tests the blood’s ability to clot
The results of these blood tests are used to calculate the Model for End-stage Liver Disease (MELD) score. Experts developed the MELD score to predict the 90-day survival rate of people with end-stage liver disease. MELD scores usually range between 6 and 40, with a score of 6 indicating the best likelihood of 90-day survival. The MELD score is used to determine whether a person is eligible for liver transplantation.
Imaging tests. Imaging tests can show signs of advanced cirrhosis, such as irregularities in the liver surface, gastric varices, and splenomegaly. These tests can also detect signs of complications, such as ascites and liver cancer.
- Ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. A specially trained technician performs the procedure in a health care provider’s office, an outpatient center, or a hospital, and a radiologist—a doctor who specializes in medical imaging—interprets the images. A patient does not need anesthesia.
- Computerized tomography (CT) scans use a combination of x rays and computer technology to create images. For a CT scan, a technician may give the patient a solution to drink and an injection of a special dye, called contrast medium. CT scans require the patient to lie on a table that slides into a tunnelshaped device where the technician takes the x rays. An x-ray technician performs the procedure in an outpatient center or a hospital, and a radiologist interprets the images. A patient does not need anesthesia.
- Magnetic resonance imaging (MRI) machines use radio waves and magnets to produce detailed pictures of the body’s internal organs and soft tissues without using x rays. A specially trained technician performs the procedure in an outpatient center or a hospital, and a radiologist interprets the images. A patient does not need anesthesia, though a health care provider may use light sedation for patients with a fear of confined spaces. An MRI may include the injection of contrast medium. With most MRI machines, the patient lies on a table that slides into a tunnel-shaped device that may be open ended or closed at one end; some machines allow the patient to lie in a more open space.
- Elastography, also called liver stiffness measurement, uses either ultrasound or MRI to measure the stiffness of the liver. Scar tissue increases the stiffness of the liver. Elastography can show how much scarring is present with some reliability. Elastography is a relatively new test. However, this test promises to be helpful in showing how severe liver scarring is and whether the scarring is getting worse over time.
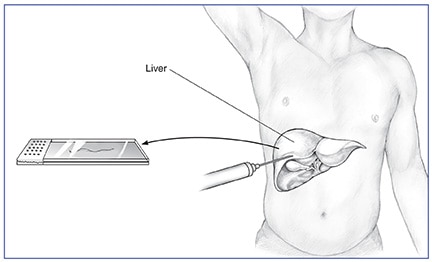
Liver biopsy. A liver biopsy is a procedure that involves taking a piece of liver tissue for examination with a microscope for signs of damage or disease. The health care provider may ask the patient to stop taking certain medications temporarily before the liver biopsy. The health care provider may ask the patient to fast for 8 hours before the procedure.
During the procedure, the patient lies on a table, right hand resting above the head. The health care provider applies a local anesthetic to the area where he or she will insert the biopsy needle. If needed, a health care provider will also give sedatives and pain medication. The health care provider uses a needle to take a small piece of liver tissue. He or she may use ultrasound, CT scans, or other imaging techniques to guide the needle. After the biopsy, the patient must lie on the right side for up to 2 hours and is monitored an additional 2 to 4 hours before being sent home.
A health care provider performs a liver biopsy at a hospital or an outpatient center. The health care provider sends the liver sample to a pathology lab, where the pathologist—a doctor who specializes in diagnosing diseases—looks at the tissue with a microscope and sends a report to the patient’s health care provider.
A liver biopsy can confirm the diagnosis of cirrhosis; however, a person does not always need this test. A health care provider will perform a biopsy if the result might help determine the cause or affect treatment. Sometimes a health care provider finds a cause of liver damage other than cirrhosis during biopsy.
How is cirrhosis treated?
Treatment for cirrhosis depends on the cause of the disease and whether complications are present. In the early stages of cirrhosis, the goals of treatment are to slow the progression of tissue scarring in the liver and prevent complications. As cirrhosis progresses, a person may need additional treatments and hospitalization to manage complications. Treatment may include the following:
Avoiding Alcohol and Illegal Substances
People with cirrhosis should not drink any alcohol or take any illegal substances, as both will cause more liver damage.
Preventing Problems with Medications
People with cirrhosis should be careful about starting new medications and should consult a health care provider before taking prescription medications, over-the-counter medications, or vitamins. People with cirrhosis should avoid complementary and alternative medications, such as herbs.
Cirrhosis slows the liver’s ability to filter medications from the blood. When this slowdown occurs, medications act longer than expected and build up in the body. Some medications and vitamins may also affect liver function.
Viral Hepatitis Vaccination and Screening
All people with cirrhosis should consider vaccination against hepatitis A and B. An infection with one of these hepatitis viruses can cause cirrhosis to get worse. Vaccination can easily prevent both infections.
People with cirrhosis should also get a screening blood test for hepatitis C.
Treating Causes of Cirrhosis
Health care providers can treat some causes of cirrhosis, for example, by prescribing antiviral medications for hepatitis B and C. In some instances, these medications cure the viral infection. Health care providers treat autoimmune hepatitis with corticosteroids and other medications that suppress the immune system. Health care providers can treat hemochromatosis and Wilson disease—inherited forms of liver disease caused by the buildup of iron or copper in the liver—if detected early. Health care providers usually treat liver diseases due to blockage or loss of bile ducts with ursodiol (Actigall, Urso). Ursodiol is a nontoxic bile acid that people can take orally. Ursodiol replaces the bile acids that are normally produced by the liver, which are toxic and build up in the liver when the bile ducts are blocked.
Treating Symptoms and Complications of Cirrhosis
Itching and abdominal pain. A health care provider may give medications to treat various symptoms of cirrhosis, such as itching and abdominal pain.
Portal hypertension. A health care provider may prescribe a beta-blocker or nitrate to treat portal hypertension. Beta-blockers lower blood pressure by helping the heart beat slower and with less force, and nitrates relax and widen blood vessels to let more blood flow to the heart and reduce the heart’s workload.
Varices. Beta-blockers can lower the pressure in varices and reduce the likelihood of bleeding. Bleeding in the stomach or esophagus requires an immediate upper endoscopy. This procedure involves using an endoscope—a small, flexible tube with a light—to look for varices. The health care provider may use the endoscope to perform a band ligation, a procedure that involves placing a special rubber band around the varices that causes the tissue to die and fall off. A gastroenterologist—a doctor who specializes in digestive diseases—performs the procedure at a hospital or an outpatient center. People who have had varices in the past may need to take medication to prevent future episodes.
Edema and ascites. Health care providers prescribe diuretics—medications that remove fluid from the body—to treat edema and ascites. A health care provider may remove large amounts of ascitic fluid from the abdomen and check for spontaneous bacterial peritonitis. A health care provider may prescribe bacteria-fighting medications called antibiotics to prevent infection. He or she may prescribe oral antibiotics; however, severe infection with ascites requires intravenous (IV) antibiotics.
Hepatic encephalopathy. A health care provider treats hepatic encephalopathy by cleansing the bowel with lactulose, a laxative given orally or as an enema—a liquid put into the rectum. A health care provider may also add antibiotics to the treatment. Hepatic encephalopathy may improve as other complications of cirrhosis are controlled.
Hepatorenal syndrome. Some people with cirrhosis who develop hepatorenal syndrome must undergo regular dialysis treatment, which filters wastes and extra fluid from the body by means other than the kidneys. People may also need medications to improve blood flow through the kidneys.
Osteoporosis. A health care provider may prescribe bisphosphonate medications to improve bone density.
Gallstones and bile duct stones. A health care provider may use surgery to remove gallstones. He or she may use endoscopic retrograde cholangiopancreatography, which uses balloons and basketlike devices, to retrieve the bile duct stones.
Liver cancer. A health care provider may recommend screening tests every 6 to 12 months to check for signs of liver cancer. Screening tests can find cancer before the person has symptoms of the disease. Cancer treatment is usually more effective when the health care provider finds the disease early. Health care providers use blood tests, ultrasound, or both to screen for liver cancer in people with cirrhosis. He or she may treat cancer with a combination of surgery, radiation, and chemotherapy.
When is a liver transplant considered for cirrhosis?
A health care provider may consider a liver transplant when cirrhosis leads to liver failure or treatment for complications is ineffective. Liver transplantation is surgery to remove a diseased or an injured liver and replace it with a healthy whole liver or part of a liver from another person, called a donor.
More information is provided in the NIDDK health topic, Liver Transplantation.
Eating, Diet, and Nutrition
A healthy diet is important in all stages of cirrhosis because malnutrition is common in people with this disease. Malnutrition is a condition that occurs when the body does not get enough nutrients. Cirrhosis may lead to malnutrition because it can cause
- people to eat less because of symptoms such as loss of appetite
- changes in metabolism
- reduced absorption of vitamins and minerals
Health care providers can recommend a meal plan that is well balanced and provides enough calories and protein. If ascites develops, a health care provider or dietitian may recommend a sodium-restricted diet. To improve nutrition, the health care provider may prescribe a liquid supplement. A person may take the liquid by mouth or through a nasogastric tube—a tiny tube inserted through the nose and throat that reaches into the stomach.
A person with cirrhosis should not eat raw shellfish, which can contain a bacterium that causes serious infection. Cirrhosis affects the immune system, making people with cirrhosis more likely than healthy people to develop an infection after eating shellfish that contain this bacterium.
A health care provider may recommend calcium and vitamin D supplements to help prevent osteoporosis.
Points to Remember
- Cirrhosis is a condition in which the liver slowly deteriorates and is unable to function normally due to chronic, or long lasting, injury. Scar tissue replaces healthy liver tissue and partially blocks the flow of blood through the liver.
- The most common causes of cirrhosis in the United States are chronic hepatitis C, alcohol-related liver disease, nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH), and chronic hepatitis B.
- Many people with cirrhosis have no symptoms in the early stages of the disease. However, as the disease progresses, a person may experience the following symptoms:
- fatigue, or feeling tired
- weakness
- itching
- loss of appetite
- weight loss
- nausea
- bloating of the abdomen from ascites—a buildup of fluid in the abdomen
- edema—swelling due to a buildup of fluid—in the feet, ankles, or legs
- spiderlike blood vessels, called spider angiomas, on the skin
- jaundice, a condition that causes the skin and whites of the eyes to turn yellow
- As the liver fails, complications may develop. In some people, complications may be the first signs of the disease.
- A health care provider usually diagnoses cirrhosis based on the presence of conditions that increase its likelihood, such as heavy alcohol use or obesity, and symptoms. A health care provider may confirm the diagnosis with
- a medical and family history
- a physical exam
- a blood test
- imaging tests
- a liver biopsy
- Treatment for cirrhosis depends on the cause of the disease and whether complications are present.
- A health care provider may consider a liver transplant when cirrhosis leads to liver failure or treatment for complications is ineffective.
- credit/source: https://www.niddk.nih.gov/health-information/liver-disease/cirrhosis
- Note: All information are all credit to original writer's sources and references.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.